
Thursday, 15 January, 2026г.
















Где искать: по сайтам Запорожской области, статьи, видео ролики
пример: покупка автомобиля в Запорожье
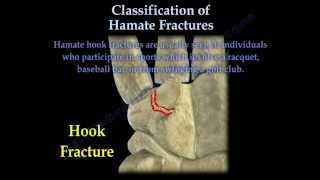
Hamate Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
 У вашего броузера проблема в совместимости с HTML5
У вашего броузера проблема в совместимости с HTML5
Dr. Ebraheim’s educational animated video describes the classification and fixation of Hamate carpal bone fractures. The base of the fifth metacarpal articulates with the hamate bone. Fractures of the hamate bone are rare, difficult to diagnose and routine x-rays may not show the fracture. Hamate fracture are classified as either a hook fracture or as a body fracture. Hamate hook fractures are usually seen in individuals who participate in sports which involve a racquet, baseball bat or from swinging a golf club. Missing the fracture can lead to persistent pain from nonunion. Hamate body fractures are associated with axial force trauma, such as a fist striking a hard object, a fall, or from crushing injuries. May also be accompanied by 4th and 5th metacarpal subluxation. Coronal fractures are the most common type of hamate body fractures. Three types of coronal fractures described by Dr.Ebraheim: •Type A: large piece •Type B: moderate piece •Type C : avulsion. Watch for subluxation of the joint. Due to the pull from the extensor carpi ulnaris. Hook fractures of the hamate are best seen by carpal tunnel or supination x-ray views. Rule out ossification center ( os hamuli proprium). For hamate fractures, CT scan is the best study. A 30-degree pronated view is helpful for body fractures. Clinical evaluation •Pain especially with axial loading of the ring and little finger or by grasping an object. •Dismissed grip strength. •May have ulnar and median nerve neuropathy symptoms. •The most common findings are pain and tenderness on the ulnar side of the wrist distal to the wrist joint. •Pain may also be felt due to compression of the ulnar nerve in the Guyon canal. Pull test is recently described •The palm of the hand is placed in supination •The wrist is in full ulnar deviation •Fingers of the patient should be flexed. •The examiner pulls on the ulnar two digits with the patient resisting the pull. •A positive test with pain in the area of the hook indicates a fractured hook of hamate injury. Treatment Acute nondisplaced fracture •Early immobilization for acute fractures with short arm splint for 6 weeks to avoid nonunion. Symptomatic nonunion •Excision of the fracture fragment •Type A and B require open reduction and internal fixation in addition to stabilization of the joint if needed. •Type C requires closed reduction and percutaneous pinning of the fragment for stabilization of the joint. •If closed reduction of the joint is not adequate, open reduction and stabilization of the joint should be done. •Displaced fragment with subluxation requires reduction of the joint and stabilization of the joint with K-wires or fixation of the fragment. •When a 5th or 4th carpometacarpal dislocation occurs, one should make a special effort to find a coronal fracture of the hamate. Become a friend on facebook: http://www.facebook.com/drebraheim Follow me on twitter: https://twitter.com/#!/DrEbraheim_UTMC
Теги:
Hamate fracture classification fixation lag screws pinning wire 5th 45h metacarpal lunate pisiform triquetrum body hook golf baseball sports racquet ball swing carpal tunnel view supination xrays scan evaluation ulnar side hand Dr. Nabil Ebraheim Nathan Elkins molly University toledo Medical Center UTMC orthopaedics surgeon
Похожие видео


Мой аккаунт